
Functional neurosurgery
- Zeljko Kojadinovic, MD- Neurosurgeon and Pain Specialist Functional neurosurgery

- Epilepsy
- Posttraumatic epilepsy
- Dyskinesias
Functional neurosurgery is the method of choice in the treatment of functional disorders of the brain when conservative methods of treatment have not yielded results. It is used for the following functional disorders: epilepsy, pain, movement disorders (dyskinesias) and psychiatric disorders.
Epilepsy
Epilepsy is a tendency for recurrent seizures. An epileptic seizure occurs due to sudden, excessive, and synchronized activity of nerve cells (neurons) in the brain, and then the functional activity is interrupted. Only recurrent seizures amount to epilepsy. One seizure is not epilepsy, and many people have at least one seizure in their lifetime (5% of the population). Everyone has an seizure threshold for the interaction of various factors that can cause epilepsy. In epilepsy, this threshold is lowered by certain factors. The incidence of epilepsy is 4-8‰ of the population. In 75% of cases, epilepsy occurs before the age of 20.
According to its etiology, epilepsy can be:
- Primary – of unknown cause
- Epilepsy that occurs within various genetic anomalies and its course is predictable. It includes: infantile and juvenile absences, juvenile myoclonic epilepsy, Lennox-Gestaut syndrome, etc.
- Secondary epilepsy is caused by damage to the brain by various diseases. These damages can include teratogenic effects, birth trauma, neurotrauma, cerebral infarction, bleeding, brain tumor, infection, inflammatory-degenerative changes, etc.
There are 30 types of epileptic seizures.
The basic division of epileptic seizures is according to whether the seizure is generalized (symmetrically moving in both hemispheres of the brain) or partial (electrical activity begins in a certain part of the brain – its focus).
| Generalized attacks | Tonic-clonic attack (grand mal or “big” attack) |
| Absance (petit mal or “small” attack) | |
| Myoclonic seizure | |
| Tonic attack | |
| Atonic attack | |
| Partial (focal) seizures | A simple partial attack – without disturbing the state of consciousness |
| Complex partial attack – with disturbance of the state of consciousness | |
| A partial attack that is secondarily generalized | |
| Unclassified attacks |
Epileptologists and neurologists deal with the diagnosis and medical treatment of epilepsy.
Diagnosis involves determining which form of epilepsy is involved and whether it is primary or secondary by origin. Many pathological processes are manifested first by epilepsy and only manifest other symptoms when they develop further. Therefore, secondary epilepsy should be ruled out after the first epileptic seizure. Therefore, an MRI scan of the brain is mandatory in diagnostic processing (a CT scan cannot detect many pathological changes in the initial phase when they only cause epilepsy). Surgical treatment of these changes can often cure epilepsy.
The diagnostic protocol includes a detailed examination, EEG, and an MRI scan of the brain. Other diagnostic methods, especially in the case of secondary epilepsy, depend on the cause of epilepsy (blood and urine lab, ophthalmological examination, cardiac treatment, pulmonary treatment).
Brain tumors are a rare cause of epilepsy in children, while for those over age 25, they are the cause in 10% of cases. More benign tumors are more likely to cause long-term epilepsy (oligodendroglioma in 80%, glioblastoma in 40%, cavernoma, meningioma, glioma, etc.).
Postoperative epilepsy is the first occurrence of seizures only after surgery.
Posttraumatic epilepsy can be:
- Initial – occurs minutes after injury. It does not tend to become permanent. Early – occurs within 7 days of injury and remains long-term in 25% of adults, and less often in children.
- Late – occurs more than 7 days after injury. 50% of posttraumatic epilepsy manifests itself within the first year. After four years, the risk of developing epilepsy is small. In 50% of cases, these are Grand mal seizures as secondary generalized focal epilepsies. There are usually more seizures, but resistant epilepsies are less common. Absences never occur due to neurotrauma. Late epilepsy occurs most often with bleeding and contusions in the brain (in 50% of cases) and depressed skull fractures (in 70%, due to a concomitant lesion of the cortex below the fracture).
If initial or early seizures occur or epileptogenic trauma occurs, an antiepileptic (usually Carbamazepine or Phenytoin) is prescribed and, if there are no seizures, the treatment is discontinued after 12 months.
Treatment aims to stop or reduce the frequency of attacks, without the patient having any side effects from the treatment. In most cases, treatment involves a change in lifestyle (avoiding situations that can provoke seizures or be dangerous if one occurs), and the use of drugs (antiepileptics). Of all patients, 60-80% will not experience any more seizures with appropriate medication. Others have so-called resistant epilepsy and in those cases treatment aims to at least reduce the number of seizures.
If the seizures recur without a break, between them, it is called status epilepticus and is an emergency.
If the attacks do not recur for a long time, the medication can be gradually discontinued. Also, if seizures occur infrequently and are caused by situations known to be provocative, treatment is not mandatory (e.g., febrile convulsions).
In refractory epilepsies, additional sophisticated testing is performed to determine if the patient is a candidate for neurosurgical treatment. The diagnostic protocol should answer the following questions:
- Is it focal epilepsy or not?
- Can its focus be detected?
- Is the focus in the temporal lobe or outside it?
- Can the surgical deficits be ruled out?
The diagnostic protocol includes:
- Detailed history and neurological examination
- An MRI scan often shows changes that are not seen on a CT scan. It can represent a focus (the origin of the epilepsy).
- EEG – interictal and ictal, as well as a 24-hour EEG (video EEG) help in focus detection. If standard methods do not reveal the focus, special electrodes can be surgically placed in the brain.
- Psychological tests
- Tests in the detection of dominant speech and memory centers. This prevents neurocognitive deficits after surgery.
Neurosurgical treatment is performed:
- If it is secondary epilepsy with a primary disease that can be operated on (tumor, brain abscess, intracranial bleeding, etc.). Often, treating the primary cause will cure the epilepsy, but not always.
- If the epilepsy is resistant to drugs (for 2-3 years, despite modern treatment), and there is a focus, it can be addressed through Functional Neurosurgery that is performed in specialized centers. The focus is the part of the brain where impulses are generated and spread further into the brain to cause an epileptic seizure. The focus is usually localized in the middle (limbic) structures of the temporal and frontal lobes of the brain, but it can be localized anywhere in its cortex. A large number of generalized seizures are generalized focal epilepsy.
There are three types of surgical treatment for epilepsy:
- Focus removal – lesionectomy, corticotomy, lobectomy, hemispherectomy (when the hemisphere is otherwise inactive after major damage in early childhood). This group of methods yields better results than the next two.
- Intersection of connections between the focus and other parts of the brain (section of corpus callosum, subpial intersection of pathways). Both methods can be performed in parts of the brain where there are no eloquent regions (brain centers whose damage would certainly cause deficits).
- Electrical stimulation, implanted stimulators, on the vagus nerve or in parts of the cerebellum that reduce the epileptic activity of the brain.
The most common neurosurgical methods in the treatment of epilepsy
Lesionectomy – involves the removal of the focus visible on the MRI scan, such as glioma, cavernoma, gliosis, atrophy of the cortex. In addition to this, if possible, several surrounding millimeters of the cortex are removed. This method is done if the lesion is outside the temporal lobe, and yields excellent results.
Resection (safe removal) of part of the temporal lobe – If a lesion is detected in the temporal lobe, a lesionectomy and resection of the temporal lobe are performed. Temporal lobe resection involves the removal of the temporal pole and hippocampus. The hippocampus is considered a frequent site of focus, and also participates in its expansion and amplification. Another variation of this operation is the removal of only the amygdala and hippocampus. Morbidity (most often speech disorder and/or quadrantanopia) after surgery is not high at about 0.5%. This operation yields the best results (good results in 80% of cases). In the event when mesial temporal sclerosis or hippocampal atrophy is visible on the MR image, healing is achieved in as many as 90% of cases.
All other methods are done less frequently and have poorer results.
Dyskinesias
Dyskinesias are treated also in functional neurosurgery. They most often manifest as excessive movements and/or increased muscle tone. The movements of body parts are regulated by an extrapyramidal system that is represented by a large number of nuclei and pathways along the entire CNS. The central place is occupied by the basal ganglia (globus pallidum, putamen and caudate nucleus).
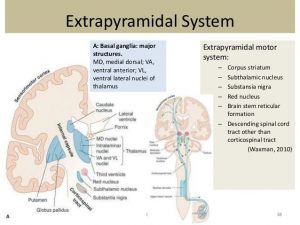
The extrapyramidal system controls the fineness and coordination of movements thanks to the fine balance between the excitatory and inhibitory function of the above-mentioned nuclei.
Medication is most frequently used in the treatment of extrapyramidal disorders. Surgical methods are used only if drugs do not work, and they aim to restore the disturbed balance. This is achieved by lesion or stimulation of individual nuclei or pathways. Today, stimulation is performed more often and involves placing an electrode in the region of the brain, and the source of impulses in the subcutaneous tissue of the abdomen. Today, Baclofen is used in the treatment of increased spasticity, which can be applied to the spinal canal with the help of special pumps that are placed under the skin, most often in the area of the abdomen. This allows lower and more precise doses of Baclofen. The following table lists the most common indications and types of operations.
| Illness- a sign | Neurosurgical method |
| Parkinson’s disease (syndrome) – tremor |
|
| Essential tremor (Tremor due to brain lesions reacts worse to treatment than essential tremor.) |
|
| Chorea and athetosis after brain lesions |
|
| Hyper spasticity after brain lesion |
|
| Spastic paraplegia of the legs |
|
| Hemiballismus |
|
| Dystonia |
|
| Spastic torticolis |
|