Zeljko Kojadinovic, MD- Neurosurgeon and Pain Specialist

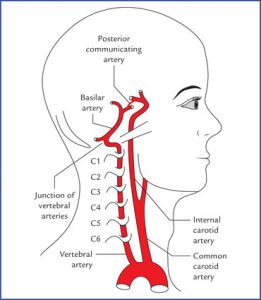
The brain is nourished by two pairs of arteries that pass from the chest through the neck to the brain. The two internal carotid arteries feed the anterior parts of the brain, and the two vertebral arteries feed the posterior parts of the brain.
Brain infarctions
Arteries feed the brain. Blood vessel diseases most often lead to an interruption of local brain circulation (when a cerebral infarction occurs) or to bleeding (such as rupture of an aneurysm). Both phenomena are popularly called “strokes.”
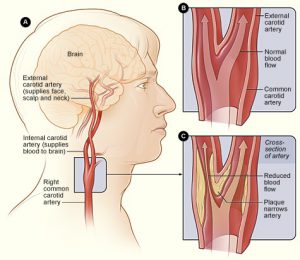
Impaired blood circulation through the brain can lead to transient disorders (TIA, VBI, RIND) or to permanent damage (brain infarction). Cerebral infarctions can be small and diagnosed accidentally on an MRI scan of the brain (especially in the elderly). This phenomenon can be mistaken for normal aging – e.g. the radiologist’s report might read “micro ischemic changes in the brain appropriate to the patient’s age.” Large infarcts lead to the extinction of a larger part of the brain and are manifested differently – weakness of the opposite half of the body, coma, visual impairment, etc. Neurologists deal with this pathology. If the patient reaches the hospital on time, the circulation through the brain can be re-established through interventions before an infarction occurs. One of the most common causes of cerebral infarction is a clot that forms on an atherosclerotic plaque that has formed on the branch of the carotid artery (located in the neck). If this plaque is large, it is treated surgically, and this operation is most often performed by vascular surgeons. When there is a massive brain infarction, brain swelling develops, compressing another part of the brain. Sometimes in that situation decompressive craniectomy is performed (temporary elimination of a big part of the skull over the infarction and widening a dura).
In addition to plaque, the causes of cerebral infarction can be plaque on the arteries of the brain, shock, very poor breathing, severe heart failure, blood disorders (e.g., anemia, polycythemia), vasospasm, vascular inflammation (vasculitis), injuries, or other diseases of the blood vessels of the brain (vasculopathy).
Brain aneurysms (intracranial aneurysms)
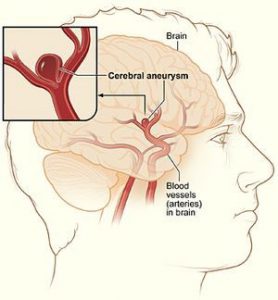
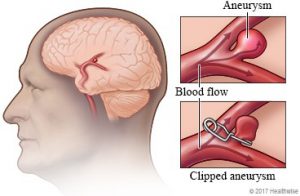
Brain aneurysms are dilations of the arteries of the brain. They usually have the shape of a sac and dimensions of 5-15 mm (although they can range from 2mm to 4cm). Children can be born with structural weaknesses in parts of the artery wall, but not with aneurysms. They appear later. They are no longer considered as rare as previously thought (occurring in 1-10% of the population). The aneurysm is most often localized on the large arteries on the lower surface of the brain. The likelihood that a close relative has also had an aneurysm is about 7-20%.
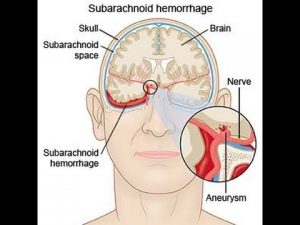
An aneurysm can remain silent for a lifetime (without manifesting any symptoms). If it manifests, it is usually because of a rupture of its wall with bleeding. It is most often in the form of subarachnoid hemorrhage (SAH) – bleeding is most often on the surface of the base of the brain. Bleeding inside the brain (brain hematoma) is also possible with or without SAH.

77% of all SAHs are caused by a ruptured aneurysm. Other reasons for this are injuries, vasculitis, coagulation disorder, art. hypertension, AVM. In 10% of SAH, no cause of bleeding was detected.

Brain aneurysm- Symptoms
Bleeding often occurs as a result of physical efforts, stress, or hypertensive crises, but also often in peace, even in sleep. Weather changes with changes in atmospheric pressure maybe can also contribute. Bleeding is most often manifested by a sudden and very intense headache. In addition to this, the patient may have nausea and vomiting, and sensitivity to light (photophobia). During the examination there is neck stiffness (meningism). If, in addition to subarachnoid, there is bleeding in the brain (hematoma), then various neurological dysfunctions occur (e.g., weakness of half of the body – hemiparesis). If the bleeding is more severe, a comatose state occurs. In about 10-15% of patients, the bleeding is so severe that they die before they arrive at the hospital.
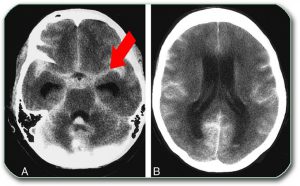
When a patient is admitted to the hospital, the clinical picture is usually clear. A CT scan of the brain is done urgently to determine the bleeding. Sometimes if it is not clear what it is about, a lumbar puncture is done to obtain cerebrospinal fluid. In cases of bleeding, the cerebrospinal fluid is bloody. In older bleeding, the cerebrospinal fluid is yellowish (xanthochromia).
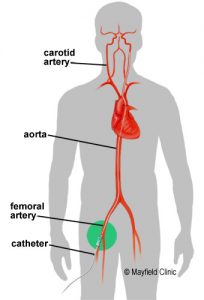
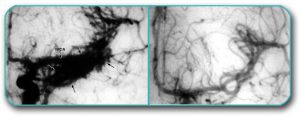
When a subarachnoid hemorrhage is detected, blood vessel imaging is usually performed urgently to detect an aneurysm. Angiography (DSA) or CT angiography (CTA) is most commonly performed.
Angiography should answer some questions:
- Was the bleeding due to aneurysm rupture?
- Are there multiple aneurysms?
- Is it necessary to operate on the aneurysm or can it be treated in another way?
- Are there complications of bleeding – most often spasms and narrowing of the surrounding arteries?
A possible replacement for DSA can be CT angiography with 3D reconstruction of arteries (imaging of brain arteries by CT imaging), and, much less often, MR angiography.
How a ruptured brain aneurysm damages the brain
Once bleeding has occurred, several pathological processes occur in parallel:
- High pressure in the cranium due to the bleeding – It is being treated with drugs. If there is a large blood clot in the brain (hematoma), the patient must be operated on urgently, and then the hematoma is removed and the aneurysm is clipped (like small clothespin, which is placed over its neck, excludes it from circulation).
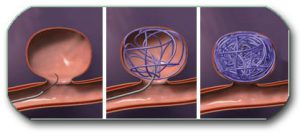
- Possibility of repeated bleeding– Bleeding from an aneurysm lasts only a few seconds. It is temporarily stopped with a weak plug of clotted blood. This plug can often loosen and there is a risk of new bleeding (60% in the first 6 weeks). Repeated bleeding (aneurysm rerupture) can be fatal. They are significantly rarer 2 months after the initial bleeding, if the patient is not operated on. In order to avoid new bleeding, we try to exclude aneurysm from the circulation as soon as possible (ideally in the first 3 days after bleeding, if the patient’s condition allows it). This can be done in 2 basic ways (see the image below). The first is to open the skull, reach the aneurysm and put a small clip on its neck (like small clothespin -see the picture below). Another method is to fill the aneurysm during angiography (DSA) with wire that coils inside the aneurysm sac. It should be filled so densely that blood can no longer enter it. The decision on the method of treatment is made by a team consisting of neurosurgeons and angio interventional specialists. In some hospitals and countries only 10% of aneurysms are operated on, while in the others about 50% are operated on. The operation itself can have complications: postoperative bleeding inside the skull, cerebral infarction, cerebrospinal fluid leakage and infections, etc. We choose to perform surgery when the risk of non-surgery is significantly higher than the risk of surgery. Yet surgery is only “half” the job in the treatment of these patients. The other half of the job involves resolving complications of the disease after surgery or coiling (they often occur regardless of whether the patient has been operated on or not). The key is to constantly monitor the patient, notice complications on time and actively treat them in the initial phase.
- Spastic narrowing of the arteries of the brain (vasospasm, angiospasm) – Arteries can become spastic. This spasm leads to a narrowing of the arteries and reduces blood flow through the brain. It starts on the 3rd day after bleeding, the biggest is 5-9 days, and can last for several weeks. The greater the bleeding, the more pronounced the vasospasm is, but it does not depend only on that. The more severe the spasm, the greater the chance of developing a cerebral infarction. Unlike the previous two processes, the treatment of spasm is non-surgical and is not as successful in more severe cases. There is currently an ongoing trial of drugs that promise to be successful in treating this condition. Also, intervention for dilatation of spastic arteries can be performed during DSA.
- Blockade of flow of cerebrospinal fluid – the possible development of “water on the brain” (hydrocephalus). The method of treatment depends on the type of hydrocephalus and is explained in the section of this site dealing with congenital malformations. If a pronounced sudden hydrocephalus occurs, it must be treated urgently. At that time we can monitor intracranial pressure (EVD- external ventricle drainage of excessive CSF).
- This type of bleeding, especially in severe cases, can lead to disorders in the work of all internal organs


Prognosis of a rupture of anurysm
All these mechanisms can lead to brain damage that can manifest in various forms. These can be minor neurological deficits (e.g. hand weakness, impaired speech, mental disorders), but also more severe damage (e.g. different degrees of depth of coma). Recovery then resembles the recovery of brain injury described on the web page “Head trauma.” Prognosis and outcome of craniocerebral injuries
A precise prognosis of damage after bleeding from an aneurysm cannot be given, especially not at the very beginning of the illness, except for cases of either very severe or very light damage.
An aneurysm can grow large and press on the brain without bleeding (giant aneurysm). It can also form blood clots that can come out of the aneurysm as emboli into the surrounding arteries and lead to a cerebral infarction.
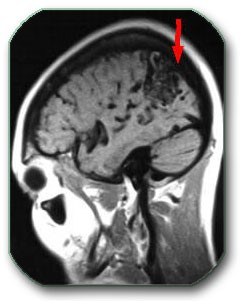
Increasingly, we are able to diagnose, especially by magnetic resonance imaging of the brain, the so-called “asymptomatic aneurysms.” They are up to 1 cm in size and do not cause any problems for the patient. The chances of them rupturing are probably less than previously thought (0.05% – 0.5% per year, depending on the size, shape, location and possible growth of the aneurysm). In these cases treatment is not urgent. Today asymptomatic aneurysms are mostly treated by coiling.
Arteriovenous malformations
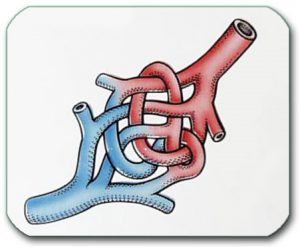
Arteriovenous malformation (AVM) is a congenital anomaly consisting of a tangle of blood vessels. One part of this formation belongs to the arterial part and the other part is the venous part. Children are born with this anomaly (unlike an aneurysm) and over time the AVM grows and can lead to surrounding cerebral infarction or bleeding.

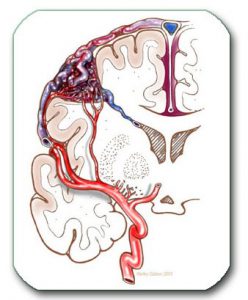



After the diagnosis of AVM, if there is no major bleeding, treatment is not urgent. The essence of treatment is that the AVM is removed surgically or occluded endovascularly or by radiation so that no more blood flows through it. If there is heavy bleeding, and the blood clot is large, it must be removed surgically. Then an attempt can be made to remove the AVM as well. Surgery immediately resolves the disease, but can sometimes be risky. In these cases, other methods of treatment are recommended: embolization during DSA or radiation with stereotactic methods (e.g. gamma knife) – see images. The first method often only reduces the AVM and usually requires a greater number of repetitions, especially if the AVM is large. With the second method, it takes 2-3 years for the AVM to disappear completely. With larger AVMs, both methods yield poorer results. Even when a small part of the AVM remains, the chance of bleeding is not significantly reduced.

AVM surgery- The entire AVM must, by complex surgery, be separated from the surrounding brain and removed. If the AVM is very large, deep and/or is next to important centers in the brain, surgery is more difficult and riskier.
If you have been given a neurosurgical diagnosis and suggested operative or non-operative treatment, you can consult us if you have any doubts. This will make it easier for you to accept the proposed treatment from your doctor and, since you have no doubts, the treatment will have a better result or you will opt for a different type of treatment. We will explain whether we think surgery is indicated, which operative methods exist, where in your country such surgeries are performed, what their risks are and how to reduce them. We will also answer all your questions.
Spontaneous bleeding in the brain
Spontaneous bleeding in the brain or spontaneous intracerebral hematomas occur most often due to the rupture of an artery with weaker walls. This weakening of the wall occurs most often due to long-term arterial hypertension. Rupture also occurs at the time of a hypertensive crisis. As a consequence of bleeding, a blood clot (hematoma) appears, which presses on the surrounding brain structures and tends to increase for several days. Depending on the size of the bleeding, the patient may have only a headache, mental changes, an epileptic seizure, weakness of the opposite half of the body, or he may even become comatose. In some patients, the first bleeding is fatal.

After an initial examination, the diagnosis is made on the basis of a CT scan of the brain. It shows the size and location of the hematoma, and possible complications (hydrocephalus, cerebral infarction, pressure on the surrounding brain). Treatment of large spontaneous intracerebral hematomas is difficult and uncertain.
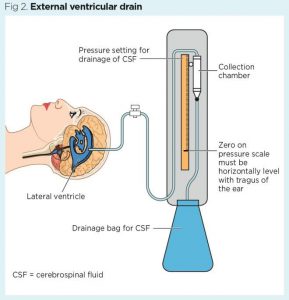
When deciding whether to operate on a patient, the primary principle is “Primum non nocere” – “First do no harm.” The decision is made based on the size and location of the hematoma, the patient’s age, the existence of other diseases, etc. If there is hydrocephalus, then EVD (externa ventricle drainage) is indicated.
Cavernoma (cavernous angioma or cavernous malformation)
A cavernoma is a formation composed of blood vessels with thin walls, in which the blood flow is not fast. The cavernoma has dimensions of between a few mm and 5 cm and can be located in the brain, cerebellum, brain stem or spinal cord. It is usually asymptomatic but can lead to epilepsy, bleeding with damage to the surrounding nerve structures (bleeding is much less frequent than with AVM), hydrocephalus, and, less frequently, other neurological damage due to growth and pressure. Neurological damage and indications for surgery depend on the location of the cavernoma, its size, whether it has bled (then it often tends to bleed again), and whether it shows growth. The diagnosis is made on the basis of an MRI scan of the brain. DSA (angiography) does not show a cavernoma. Treatment is operative and is indicated if the cavernoma is accessible, and especially if the above-mentioned characteristics are present (bleeding, drug-resistant epilepsy, neurological deterioration, etc.). It often takes two or more MR imagings to make a decision about surgery. Stereotactic radiation (e.g. Gamma Knife) in cavernomas has not produced satisfactory results.![]()
Hemangioblastoma
Hemangioblastomas are highly vascularized tumors. They occur most often in the area of the cerebellum and there are often large cysts around them. The cysts usually exert the greatest pressure on the nervous tissue. When diagnosing hemangioblastomas, it is important to exclude Von Hippel Lindau disease.