The division of the spinal column is shown in the following figure.
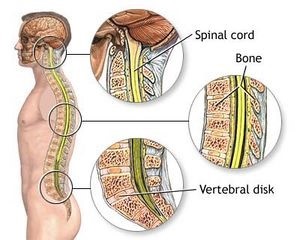
The following picture shows a cross section of the spine. The spinal column is formed of 33-35 vertebrae. The spinal canal contains the spinal cord and nerve roots (cervical and thoracic spine) or simply the nerve roots (cauda equina in the lumbar part of the spine).Figure: Anatomical elements of the thoracic spine
According to the localization, spinal tumors can be divided into:
Tumors growing from the vertebrae (anterior or posterior part of the vertebrae) – the most common are chondroma, osteoma, osteoid osteoma, chordoma
Tumors that grow inside the dural membrane but outside the spinal cord – the most common are neurinoma (growing from the root of the spinal nerve) and meningioma (growing from the dural sheath)
Tumors that grow inside the spinal cord – the most common are astrocytomas and ependymomas.
Many malignant tumors of other organs can metastasize to the spinal canal or vertebrae. Vertebral metastases are often seen on skeletal scintigraphy.
Figure: A. Tumors growing from the vertebral body; B. Tumors growing from the posterior parts of the vertebrae; C. Tumors growing inside the dural membrane but outside the spinal cord; D. Tumors growing inside the spinal cord. E. Cusa – a device that removes tumors.
These, as well as other tumors in the body, occur due to changes (mutations) in special genes of normal cells. By mutation, some genes become active (proto-oncogenes become oncogenes), and others are inactivated (tumor suppressor genes). This happens continually in the body in many cells, but the immune system recognizes these cells and neutralizes them. Sometimes these cells are not neutralized and, if they continue to multiply, a tumor is formed from them. It is usually benign at first, but over time it can accumulate an increasing number of these genes and so the tumor can become more malignant.
The reasons for these gene changes are not always known. Mutations can be the result of the action of some viruses, which have previously caused minor infections; radioactive radiation; or some chemicals (there is growing proof that various pesticides and even food additives can be carcinogens). Almost no brain tumor is directly inherited, but the offspring of people who have had malignant diseases may have inactivated proto-oncogenes, or a weaker immune system, etc. However, the influence of some factors, such as radiation from mobile phones (especially on children), radiation from high-voltage electrical cables, frequent X-rays, some medications, head injuries, poor diet, etc., are still being investigated.
These tumors are divided into benign and malignant according to how quickly they progress and in what percentage of cases they can be cured. Based on their growth, tumors can be divided into those that only press on the spinal cord (meningiomas, neurinomas, metastases, etc.) and those that infiltrate them (astrocytomas, ependymomas, malignant tumors, etc.), and combined.
Image: Tumor within the dural membrane of the spinal cord
When the tumor reaches a significant size, it exerts surrounding pressure on the spinal cord and nerve roots and leads to their swelling, disrupts blood flow in the nervous tissue, and can even lead to bleeding. The mechanisms by which the tumor damages nerve tissue are numerous and interconnected.
All this results in symptoms such as:
Pain in the spine, arms, body, or legs
Numbness of certain parts of the body
Limb weakness
Urination and stool impairment
Less often, tumors in the upper part of the spine can cause problems with breathing
Spinal tumors can also cause vertebral fracture and consequent spinal instability (malposition between vertebrae).
In benign tumors, one or more symptoms appear first, and then for months, and often years, no new symptoms appear, even as the tumor keeps growing. The above-mentioned symptoms, due to slow growth, often appear only when the tumor grows significantly.
Since small tumors are much easier to treat than large ones, it is important to diagnose tumors as soon as possible.
The most important diagnostic method is magnetic resonance imaging (MRI) of the brain. Thanks to widespread availability, this recording should be done at the first symptoms that indicate that there may be a tumor. This recording is painless and lasts about 15-45 minutes. It involves the patient lying in the narrow space of a device and being exposed, to a greater or lesser extent, to noise. This can be so uncomfortable for some people that it must be done under sedation or anesthesia (through previous administration of tranquilizers or sleeping pills). Usual intravenous contrast (non-iodine contrast) should be administered.
When analyzing the MR image, it is especially important to exclude multiple sclerosis (sclerosis multiplex) or various inflammatory changes in the spinal cord (e.g., transverse myelitis).
In addition, other diagnostic methods may be indicated, such as X-ray of the spine, computed tomography (CT), electromyography (EMG), somatosensory evoked potentials (SSEP), or imaging of the spine after administration of radioactive materials (skeletal scintigraphy).
Imaging of other organs (oncological treatment) must always be done to investigate the possible existence of other tumors in the body. It is also important to determine if the patient is suffering from other diseases. This can be important when planning anesthesia and choosing treatment methods. Minimum testing requirements are: laboratory processing of blood and urine, ECG, X-ray of the lungs, ultrasound of the abdomen and examination by an internist. Additional examinations can be performed if necessary: urological, cardiological, gynecological, etc.
methods.
Image: MR image – Black arrow shows neurinoma of the thoracic spineImage: MR image of the spine shows a tumor of the spinal cord (ependymoma – red arrow) which causes the appearance of cysts inside the spinal cord above and below itself (yellow arrow).
When a spine tumor is diagnosed, a team of experts (a neuro-oncology team) considers possible courses of treatment for the patient. We have at our disposal: symptomatic, surgical (tumor surgery) and adjuvant treatment. The decision on how to treat a patient is made based on knowledge and experience in neuro-oncology.
In some cases, especially in the elderly and people who are more seriously ill with other diseases, we decide to simply monitor the tumor (through periodic MR or CT scans).
If you have been given a neurosurgical diagnosis and suggested operative or non-operative treatment, you can consult us if you have any doubts. This will make it easier for you to accept the proposed treatment from your doctor and, since you have no doubts, the treatment will have a better result or you will opt for a different type of treatment. We will explain whether we think surgery is indicated, which operative methods exist, where in your country such surgeries are performed, what their risks are and how to reduce them. We will also answer all your questions.
Surgical treatment
If the tumor is not malignant and does not grow widely infiltratively, the goal is always to remove the entire tumor. In cases where the tumor infiltrates the vertebrae and the surrounding soft tissues, that tissue is often removed, as well as the marginal tissues around the tumor. If the tumor infiltrates the spinal cord (benign astrocytoma, and especially malignant astrocytoma), removal of the surrounding tissues (parts of the spinal cord) is not possible.
The operative approach to the spine, as in the operation of degenerative diseases of the spine, can be from the front and from the back. If the tumor grows on the vertebrae (bone tumors), then the tumor and that part of the vertebrae are removed. There are 2 basic types of surgery – laminectomy (removal of the posterior part of the vertebra) and corpectomy (partial or complete removal of the vertebral body).
Figure: A1, A2, and A3 show various degrees of vertebral lamina removal (laminectomy); Figures B1, B2, B3, and B4 show the various degrees of vertebral body removal (corpectomy); Figures C1 and C2 are a combination of the previous two types of operations.Image: A tumor in the posterior part of the vertebra (lamina) before and after surgery.
Sometimes the tumor and/or surgery lead to spinal instability and after the tumor is removed, vertebral stabilization at that level is required.
Figure: X-ray of the spine after removal of the vertebral body tumor (as in Figure B4)- the red arrow shows the prosthetic replacement for the removed vertebral body. The yellow arrow shows the posterior stabilization of the vertebra
Often, metastases in the vertebral body lead to its fracture by the type of compression fracture, which can lead to kyphotic curvature of the spine. These further damages the spinal cord and nerve roots. In these cases, palliative surgeries like vertebroplasty or kyphoplasty are also considered. During this operation, the tumor is not removed, but rather cement or other material is injected into the vertebral body under pressure through a special needle and syringe, with minimal invasiveness. This (mostly kyphoplasty) increases the height of the vertebral body and establishes a normal curvature of the spine. This results in a reduction in pain and contributes to the recovery of the spinal cord, if it was not significantly damaged. This operation is indicated in severe patients or in those for whom, with later radiation, the growth of metastasis can be regulated.
Image: Thoracic spine vertebral tumor that led to bone weakening and, subsequently, vertebral body collapse (compressive pathological fracture)Image: Vertebroplasty, where a needle is inserted into a collapsed vertebral body. Under pressure, cement is injected to restore its heightImage: KyphoplastyPicture: Malignant tumor (chondrosarcoma) of the vertebral body
A few days after the operation, pathohistological analysis of the tumor tissue is done (PH analysis – preparations are made with special stains of the sections, which are examined by a pathologist under a microscope). Experts then decide whether additional treatment with radiation and/or cytostatics is needed.
Adjuvant treatment methods are radiation and chemotherapy.
Radiation therapy is most often performed using radiation devices that have different degrees of precision. Standard radiation therapy is performed in multiple sessions (30 to 70), going through different parts of the brain each time. This way, the tumor receives by far the highest doses of radiation (dosage is measured in Grays – Gy). The most precise radiation is achieved by using radiosurgical methods (Gamma knife, Linac, cyber knife, etc.). Such precise radiation can stop the growth of tumors if they are no larger than 2.5-3.5 cm in diameter and are not very close to brain structures that do not tolerate radiation. They can also stop the growth of smaller parts of the tumor that are left behind after the operation.
We are generally not against these alternative methods, they should always be discussed with experts. This is not to discourage the patient from trying them, but to prevent alternative therapists from affecting the results of classic medical therapy. There have been instances where the alternative therapist makes changes to the primary treatment, administers treatment that the patient has already received, or promotes drugs or substances that have not been clearly shown to be effective or even some that are harmful.
The prognosis after treatment depends mostly on the type of tumor (worse in infiltrative and malignant tumors), the severity of neurological damage, and MRI scan of the spine (severity of spinal cord damage and changes in it, and possible tumor remnants – tumor residues).
Specifics of individual tumor types
Spinal meningioma
is localized in the spinal canal. It arises from the cells of the spinal cord sheath and is attached to it (dura mater). Symptoms include: local pain radiating in dermatomes, weakness, and numbness in the part of the body below the tumor site. The diagnosis is made on the basis of an MRI scan. The operation is almost always performed with a back approach and the spinal canal is entered by removing the posterior part of 1 or more vertebrae, as in Figure A2 (laminectomy, laminotomy). Meningioma can be completely removed without causing additional damage. If diagnosed in time, after the operation, the patient should make a complete recovery. A malignant variant of this tumor is rare.
Spinal neurinoma, schwannoma
It is localized in the spinal canal. It arises from the cells of the roots of the spinal nerves (radix) and is attached to it. The clinical picture includes local pain radiating in dermatomes, weakness, and numbness in the part of the body below the tumor site. The diagnosis is made on the basis of an MRI scan. The operation is almost always performed with a back approach and the spinal canal is entered by removing the posterior part of 1 or more vertebrae, as in Figure A2 (laminectomy, laminotomy). Neurinoma can be completely removed without causing further damage. If diagnosed in time, the patient should make a complete recovery after the operation. A malignant variant of this tumor is rare.
Spinal cord glioma (astrocytoma, ependymoma)
These tumors are localized within the spinal cord. Cysts in the spinal cord (syringomyelia) are often present above or below them. The clinical picture includes pain, weakness, and numbness in the part of the body below the tumor site. The diagnosis is made on the basis of an MRI scan. The operation is almost always performed with a back approach and the spinal canal is entered by removing the posterior part of 1 or more vertebrae, as in Figure A2 (laminectomy, laminotomy). Astrocytomas have a higher potential to permeate the brain (infiltration), and therefore some of these tumors cannot be completely removed. The malignant variant of these tumors is most often in the form of anaplastic astrocytoma. Malignant variants are more common than in neurinoma and meningioma, but less common than brain gliomas.
Tumors of the vertebrae
These tumors may involve the anterior or posterior portions of 1 or more vertebrae. They can grow into and/or out of the spinal canal (paraspinal tumors). When they grow into the spinal canal, they can cause damage to the spinal cord or nerve roots at that level. In addition, they can lead to vertebral fractures (so-called pathological fractures). This can then lead to instability and damaged curvature of the spine. There are a large number of tumors of the spinal vertebrae that are divided according to the tissue from which they arise: chordoma, chondroma, osteoma, osteoid osteoma, osteoblastoma, vertebral body angioma, eosinophilic granuloma, fibroma, etc. Malignant variants of these tumors are called sarcomas.
The diagnosis is made on the basis of X-rays, and CT and MR images of the affected part of the spine. Treatment is mostly operative and the spine is approached from the front or from the back. Infiltrated parts of the vertebrae are removed as in the picture above. Stabilization as in the picture above is also often required.