Congenital anomalies of the nervous system are either the result of teratogenic influences during intrauterine development (viruses, chemicals, radiation), or occur due to hereditary genes. They can be of varying degrees. They are often associated with other anomalies. If they are large, they are noticeable during fetal ultrasounds during pregnancy. Sometimes the anomalies are of such a degree that termination of the pregnancy is advised. If they are smaller, they can manifest later in life or they may not manifest at all.
Hydrocephalus
Hydrocephalus is an accumulation of cerebrospinal fluid in the ventricles of the brain. The cerebrospinal fluid is the fluid that is located in the cavities of the brain (ventricles) and around the entire brain and spinal cord. It is produced in the ventricles, flows in and around the brain and is resorbed in intracranial veins. If there is an obstacle to its continuous flow and resorption from the brain, it accumulates, leading to the expansion of the ventricles and pressure on the brain tissue. Causes of obstructions of the cerebrospinal fluid flow can include congenital obstructions, tumors, bleeding, infections, adhesions, etc.
Clinically, we distinguish between two basic types of hydrocephalus:
Hydrocephalus in children
Hydrocephalus in adults.
Hydrocephalus in children in the first and second year is manifested by an enlargement of the head, the eyes show a whitishness between the iris and the eyelid (which is not normal), the child vomits, has a tense fontanelle and does not progress in development. The diagnosis is made on the basis of an ultrasound image through the fontanelle and an MR-CT image of the brain. It is mainly treated surgically. There are two basic categories of surgical methods. Endoscopic intervention opens the floor of the third ventricle, if there is an obstacle to the outflow of cerebrospinal fluid between the ventricles, in order to bypass the obstacle. Another method involves placing a system of tubes that redirects the excess cerebrospinal fluid into a body cavity where it returns to the bloodstream (most often the abdominal cavity, through a ventriculoperitoneal shunt, VP shunt). It is important not to drain too much cerebrospinal fluid. Valves of different resistance help us ensure that that does not happen (variable-programmable valves or valves of constant resistance).
Picture: Child with hydrocephalus – the head is enlarged, the veins on the head are pronounced, and the child does not progress in development.Picture: On the left is a view of a man with brain cavities (ventricles) of normal size, and on the right with dilated ventricles due to the hydrocephalusFigure: Endoscopic intervention opens the floor of the third ventricle. It can be done if there is an obstacle to the outflow of cerebrospinal fluid between the brain ventricles (mostly between the 3rd and 4th ventricle), to bypass this obstacle.Picture: A ventriculoperitoneal shunt, by which the excess fluid from the ventricles of the brain is gradually drained into the abdominal cavity where it goes into the blood.Hydrocephalus in adults is manifested initially by mental deterioration, difficulty with walking, and involuntary urination. In addition, there may be instability, headaches and other symptoms. If hydrocephalus is caused by a disease (tumor, bleeding), the symptoms of that disease can dominate and mask the signs of hydrocephalus. The diagnosis is made on the basis of a CT or MR image of the brain, and additional analyses.
Normal-pressure hydrocephalus is a special type. It can develop over the course of months and years with slow mental decline, gait and urination disorders. Most patients suffering from it are diagnosed with senile dementia, Alzheimer’s disease, poor blood circulation through the brain, and/or cerebrovascular insufficiency. It is important to recognize this condition because in cases of normal pressure hydrocephalus, many patients with mental decline and dementia can be helped (Alzheimer’s, or senile dementia).
Treatment of hydrocephalus is usually surgical. In most cases, if there is an obstruction that can be operated on, its removal immediately eliminates the hydrocephalus. If surgery is needed, it is performed similarly to the method of surgery in children. A ventriculoatrial shunt is also often inserted. This shunt also connects the ventricles of the brain and the atrium of the heart with a system of tubes, through which the excess cerebrospinal fluid is drained.
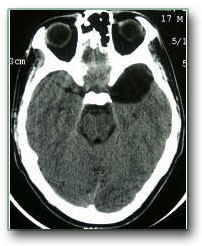
Image: An MRI scan on the left shows very enlarged ventricles of the brain. (Senile dementia may look similar). The image on the right shows what normal ventricles look like (arrows show chambers).Image: CT scan of the brain. The arrow shows a colloid cyst that prevents the flow of cerebrospinal fluid and causes the ventricles to expand (hydrocephalus). When it is removed, it will probably eliminate hydrocephalus without additional treatment
Arachnoid cyst
An arachnoid cyst is a cystic formation filled with cerebrospinal fluid (clear fluid found in the brain cavities and around the brain). The walls of that cyst consist of one of the meninges (arachnoid). Arachnoid cysts are common, but their treatment is rarely indicated, especially surgical. Many people have congenital defects in certain parts of the brain that do not manifest themselves in any way (the vast majority of patients are mentally healthy, with normal intelligence and no neurological deficits). These brain defects are filled by cerebrospinal fluid and thus an arachnoid cyst is formed. They are more often localized to the temporal region, around the optic nerves and behind the cerebellum. They are most often discovered by chance when the patient, due to other ailments, goes for a CT or MRI scan of the brain (e.g., headache, dizziness). This most often worries the patients. However, in over 99% of cases this cyst is an incidental finding and requires no treatment.
In rare cases, the cyst grows or puts pressure on the surrounding brain. Then it is usually treated surgically very successfully. The key to the operation is to drain it into another space. Communication with the subarachnoid space can be achieved surgically or with an endoscope. Another method is to place a tube in the cyst to drain the cerebrospinal fluid from it. As with hydrocephalus, it can be drained into the abdominal cavity.
Images: MRI and CT scans of the brain show a temporal cyst that does not require any treatment
Chiari malformations (Arnold-Chiari malformation)
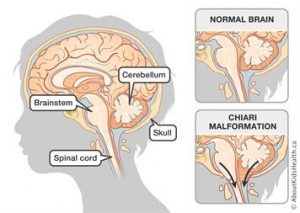
Chiari malformation involves the congenital lowering of parts of the cerebellum (cerebellar tonsils) into the spinal canal in the neck. These parts of the cerebellum put pressure on the nerve structures there – the spinal cord, nerve roots, and arteries. It causes pain in the neck and nape, especially when bending the head, also weakness in the arms and legs and dizziness. In addition to this, a cavity can be formed in the spinal cord that causes additional pressure (syringomyelia). Hydrocephalus can also occur.
The disease can manifest at birth, when it has a poor prognosis. Milder forms are manifested from childhood until old age, when they can be successfully treated surgically. The essence is to widen the opening, through which parts of the cerebellum pass, so that they exert no pressure on the above-mentioned structures. After this operation, the cavity in the spinal cord, and often the hydrocephalus, usually go away on their own. There are borderline lowering of the cerebellar parts into the spinal canal which must be carefully analyzed by an expert to determine if they require surgery or should just be monitored.
Figure: The arrow on the MR image of the brain shows the lowering of the lower parts of the cerebellum into the spinal canal, where they put pressure on the spinal cord and nerve rootsImage: A part of the cerebellum (tonsils) descends into the spinal canal and puts pressure on the surrounding structures.
Encephalocele
Meningocele is a defect on the skull through which a “ball” of fibrous brain coverings (dura) with fluid in it protrudes. If there is nervous tissue in that ball it is called encephalocele. These changes may be at the base of the skull or above at the convexity of the skull. They can be seen as an outgrowth from the skull during an ultrasound examination of the uterus or at birth. Smaller encephalocele and skull-based ones do not have to be noticed immediately. Treatment is usually neurosurgical. The outcome depends on the extent of the damage to the brain tissue and whether there are other anomalies.
Figure: Surgery on a child with occipital encephalocele.
Craniosynostosis
Craniosynostosis means premature fusion of the skull bones (before the 8th month) which halts the development of the skull, due to which the brain cannot develop properly after birth and suffers from pressure. In more serious cases the child must be treated surgically.
Spinal malformations
Spinal malformations are also numerous. Spina bifida is common. It is a condition where there is no fusion of the back part of the vertebrae. It usually does not cause any symptoms. However, parts of the dura with cerebrospinal fluid (meningocele) or even with nerve elements (myelomeningocele) can prolapse through this defect. They usually manifest at birth and are especially dangerous for those with a skin defect.
Image: Spinal meningocelePicture: A newborn with meningomyelocele.Tethered cord syndrome is a congenital malformation which causes a pulling and tightening of the lower part of the spinal cord (below the level of the L1-L2 vertebrae). It causes weakness of the legs. The disease can be manifested in children or adults as weakness of the legs, numbness, tingling, or urinary or stool disorders. It is diagnosed by magnetic resonance imaging of the spine. It is important to rule out other anomalies. It is treated surgically.
Figure: Tethered cord syndrome in which the end of the spinal cord is pulled to the level of the L5 vertebra (red arrow). Normally this end is at the level of the L1 or L2 vertebrae.Dermal sinus is a canal from the surface of the skin to the spinal canal.


 Image: Brain anatomy
Image: Brain anatomy